Excess Mortality - A Better Estimate of COVID-19 Deaths
Brian Murphy
December 4, 2020
This video is 13 minutes in duration.

Excess Mortality - A Better Estimate of COVID-19 Deaths
Brian Murphy
December 4, 2020
This video is 13 minutes in duration.
Transcript
Hello. I’m Brian Murphy and I want to present you with the real death rate from COVID-19, which is substantially lower than what is being reported by the Center for Disease Control, CDC. For the week ending November 30, 2020, the CDC reported that 244,354 people in the USA have died of COVID-19. The CDC points out that this figure is lower than the figure from other media outlets because of two or more weeks delay in collecting death certificate data. Johns Hopkins reports 266,895 deaths as of November 30, 2020. By analyzing excess mortality, we shall show that both of these figures are grossly exaggerated. We already know that both of these figures may be very high due to confusion or uncertainty in assigning the cause of death. We also know that institutions that are financially incentivized to declare COVID-19 as the cause of death, may be doing just that, especially in the presence of multiple co-morbidities, any one of which may have been the primary cause of death. In the midst of confusion, there is a financial incentive to choose COVID-19 over other causes. Finally, even without financial incentives and with the best intentions, determining the cause of death in some situations can be clinically difficult to ascertain.
The concept of “excess mortality’ is very useful in providing a method of examining death data in a way that is totally free from the complexity of co-morbidities and the errors from financial bias or clinical evaluation in writing death certificates. Excess mortality is simple. Excess mortality is the number of deaths that occur from all possible causes in a given time period that exceed the number of deaths that normally can be expected to occur in the same time period. It is simply the arithmetic difference of two numbers – total deaths from death certificates minus projected deaths from the historical trend. This method assumes one fact to be true that most people are willing to accept – all death certificates represent real deaths, irrespective of the cause. The reason why looking at excess mortality is helpful in ascertaining the impact of a pandemic is that the normal death rate, without a pandemic, for an entire nation like the USA, does not vary by much more than 1% from year to year. Therefore, a sudden increase in deaths that is much larger than 1% is detectable and attributable to some new cause, such as a pandemic. If all other factors leading to death such as automobile accidents, homicides, suicides, pneumonia and other causes are relatively constant, one can surmise that excess mortality approximates the actual number of COVID-19 deaths. Or, if one proposes that COVID-19 deaths were associated with a decrease in deaths from other causes, implying that there is a subset population that would have died anyway from other causes, without COVID-19, excess mortality still provides an estimate of the total number of people who would not have died without the COVID-19 pandemic. As such, excess mortality represents the true new additional death burden on society and is therefore useful for determining public policy for a pandemic.
CDC Publishes Excess Mortality
On October 23, 2020, Rossen et al from the CDC published a detailed analysis of excess mortality entitled "Excess Deaths Associated with COVId-19, by Age, Race and Ethnicity – United States, January 26-October 3, 2020." They reported an excess mortality of 299,028 for the stated analysis period of 36 weeks, which is less than one full year. However, they averaged the previous five years of death rates to come up with a death rate projection for 2020. We take serious issue with this averaging method. This method effectively biases the projection of 2020 deaths, without COVID-19, downward, making the resulting excess mortality high. The effect is very substantial.
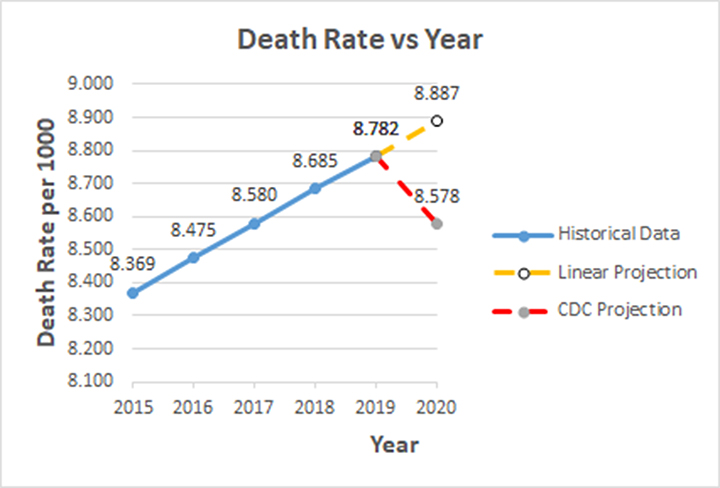
We obtained historical death rate data from Macrotrends historical death rate, wherein one sees from their graph that the death rate has been increasing linearly for the past five years. To illustrate the bias even more clearly, we re-plotted the historical known death rate data. The graph shows how the death rate increased linearly from 2015 to 2019, most likely due to the aging population. Hence, to obtain a death rate projection for 2020, it is logical to simply extrapolate that rate to 2020 (8.887 per thousand) as shown by the orange dashed line labelled “Linear Projection”.
Here is a little side bar to help you become familiar with the death rate numbers. A death rate of 8.887 per thousand per year is equivalent to 0.89% per year. So, multiplying that by the total population of the USA, 331,531,123 yields an annual death count from natural causes of 2,946,516. That is 8,072 per day! So when the mainstream media announces that 1,200 people died from COVID yesterday, you should believe that 1,200 people died. That is still much less than the natural normal daily death toll of 8,000. But you should question whether they died from COVID-19 or from other natural causes and are simply a mislabeled sub-group of the natural daily deaths.
Back to the chart. The CDC projection is shown by the red dashed line. The CDC projection for 2020 is the average of the death rates from 2015 to 2019 (8.578). It is clear from the graph that this average is a significant underestimate. It actually corresponds to the death rate in 2017. It is even much less than the value in 2019 (8.782). To say that the projected death rate in 2020 (without COVID-19), is less than it was in 2019, given the obvious upward trend, is absurd. The CDC authors admit to all the possible sources of error and to the fact that results vary based on different methods of calculation. They are not naïve. Nevertheless, their analysis is seriously biased. This bias alone makes the CDC excess mortality 198,801. Based on the linear projection, the excess mortality for the analysis period is 127,835 – much lower.
There is more CDC bias. The CDC analysis also introduces and applies weighting factors, which are described but not specified in detail, to increase the number of actual deaths based on estimates of under-reporting or late reporting. This has the effect of substantially increasing the excess mortality by 100,227 to 299,028. This is huge. It is more than double our value of 127,835. There is no need to correct for late reporting of natural deaths because the late reporting of early January natural deaths would cancel with the late reporting of late October natural deaths. Admittedly, there are more late reports of COVID-19 deaths in October than in February. Yet, how can a correction factor of 100,227 (78%) COVID-19 deaths ever be justified? Unexplained correction factors, if used, should be small – not 78%. So, the CDC projection of excess mortality is again biased by dubious correction factors to death counts, further undermining confidence in the analysis. The CDC excess mortality is biased upward by 134% to 299,028!
Public Policy Implication
We estimate the excess mortality in the USA, for the period of January 26 to October 3, 2020 (36 weeks) to be 127,835. The implications of this large discrepancy from the CDC estimate of 299,028 can be substantial in considering public policy. An excess mortality of 127,835 likely means that actual COVID-19 deaths for the analysis period are closer to 127,835, much less than CDC estimate of 299,028.
What other factors could influence excess mortality? Anecdotal evidence suggests that mortality due to non-COVID-19 causes has increased during the pandemic. For example, suicides, drug over doses, delayed cancer diagnoses, delayed cardiovascular therapy, delayed stroke therapy, delays in every health delivery in every category have all increased, making the COVID-19 portion of excess mortality somewhat lower. On the other side, reduced auto fatalities makes COVID-19 fatalities somewhat higher than the excess mortality. There is no real data to correct for all of these factors. If we assume that they cancel each other out, excess mortality remains our best estimate of COVID-19 deaths - 127,835 for the defined period of January 26 to October 3, 2020.
If we compare this current excess mortality to the deaths from the Asiatic flu of 1958 (115,000) and prorate that number to 230,000 deaths to correspond to a doubling of our population since 1958, we can conclude that COVID-19, with an excess mortality of 127,835 is much less deadly per capita than the Asiatic flu of 1958. In 1958 there were no lockdowns, no mask mandates, no mandated disruption of public schools, no disruption of school sports and no mandated major disruption of the economy. Personally, at age 15, I was very sick for three weeks with the Asiatic Flu. We should have just done today what we did in 1958 – quarantine the sick and take care of them. This jibes well with the advice of thousands of physicians who signed the The Great Barrington Declaration wherein the doctors criticize lockdowns, argue for “focused protection” of the vulnerable and a return to normal life.
On November 2, 2020, I wrote an email to the lead author on the CDC article, Dr. Lauren Rossen. I presented my analysis of excess mortality and invited her to comment. Four weeks later, as of December 1, 2020, I have not received a reply.
For the more recent period of January 26, 2020 to November 28, 2020, (44 weeks) we compute an excess mortality of 2,602,812-2,493,205=109,607, a slight drop that is within the variability of the method.
If excess mortality was used by the mainstream media to estimate COVID-19 deaths and then presented to the public, most people would be convinced that the current lockdown treatment of society is an hysterical response that is far worse than the disease itself. I urge policy makers to quarantine the sick and to stop quarantining the healthy. Lockdown is tyranny! Demanding that others suffer in an effort to save lives is feigned humanitarianism and pure hypocrisy. If one feels compelled to save lives, work to eradicate abortion where 800,000 lives can be saved annually in the USA alone and 10 million worldwide.
Projected deaths at 36 weeks = 331,539.123 x (36/52) x 8.887384/1000 = 2,039,895
Excess mortality = 2,167,730 - 2,039,895 = 127,835
Question: email me at brian@godsplanforlife.org.